Case Summary
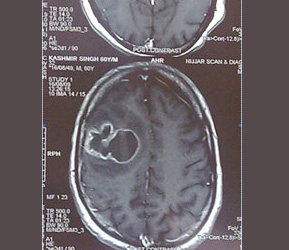
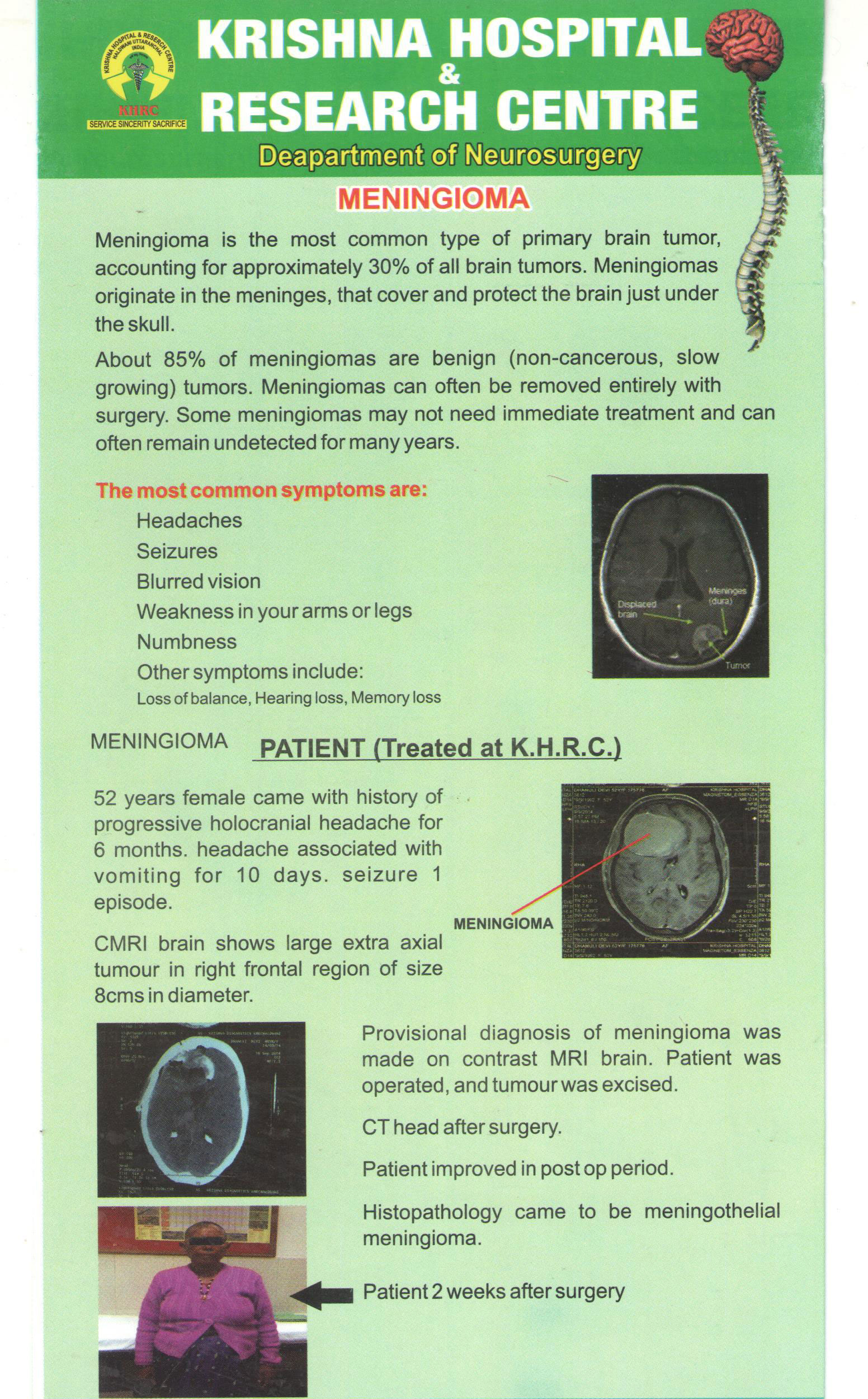
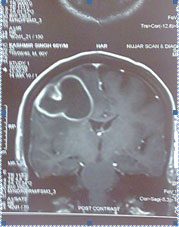
MRI BRAIN of patient showing abscess in brain
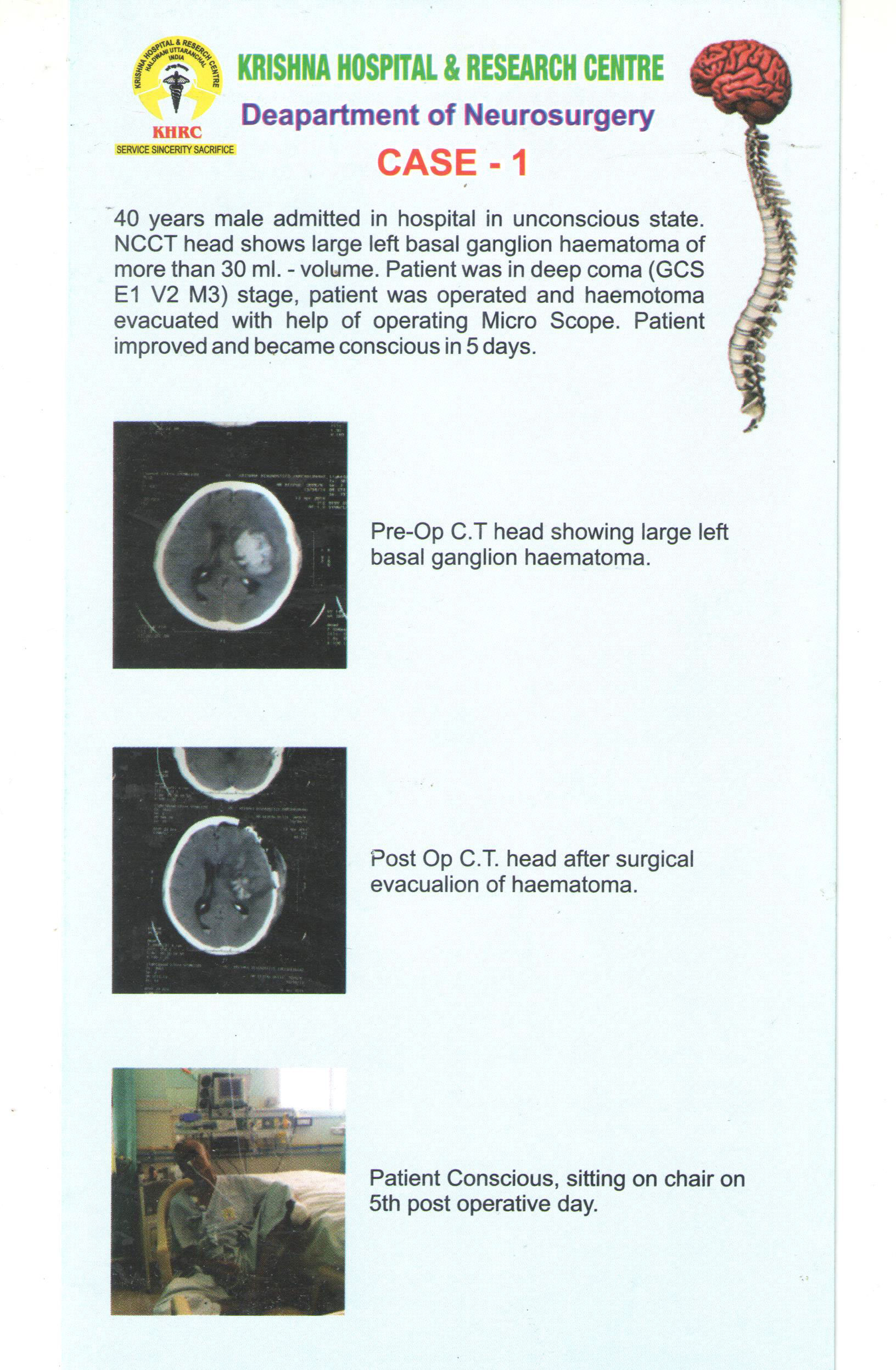
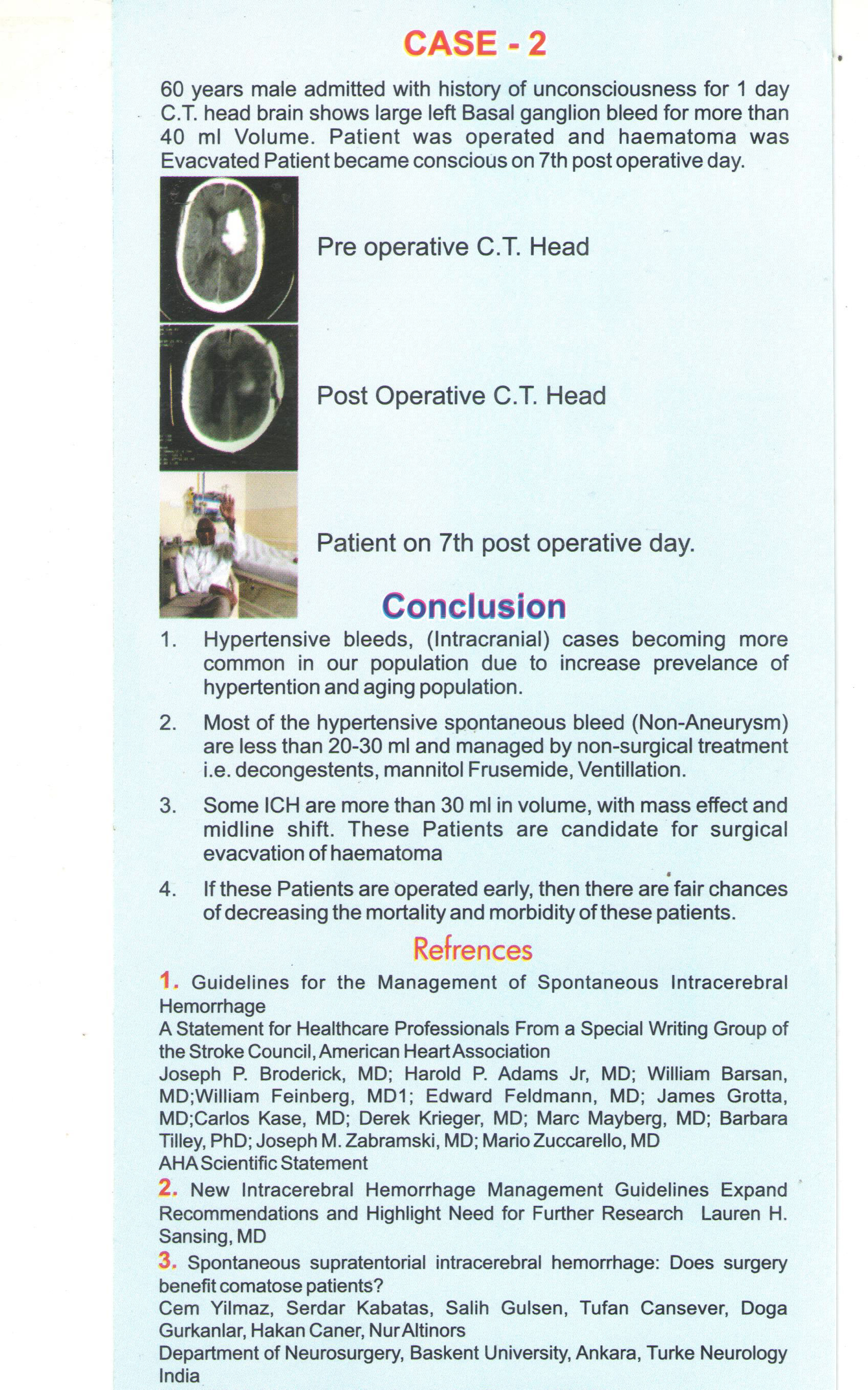
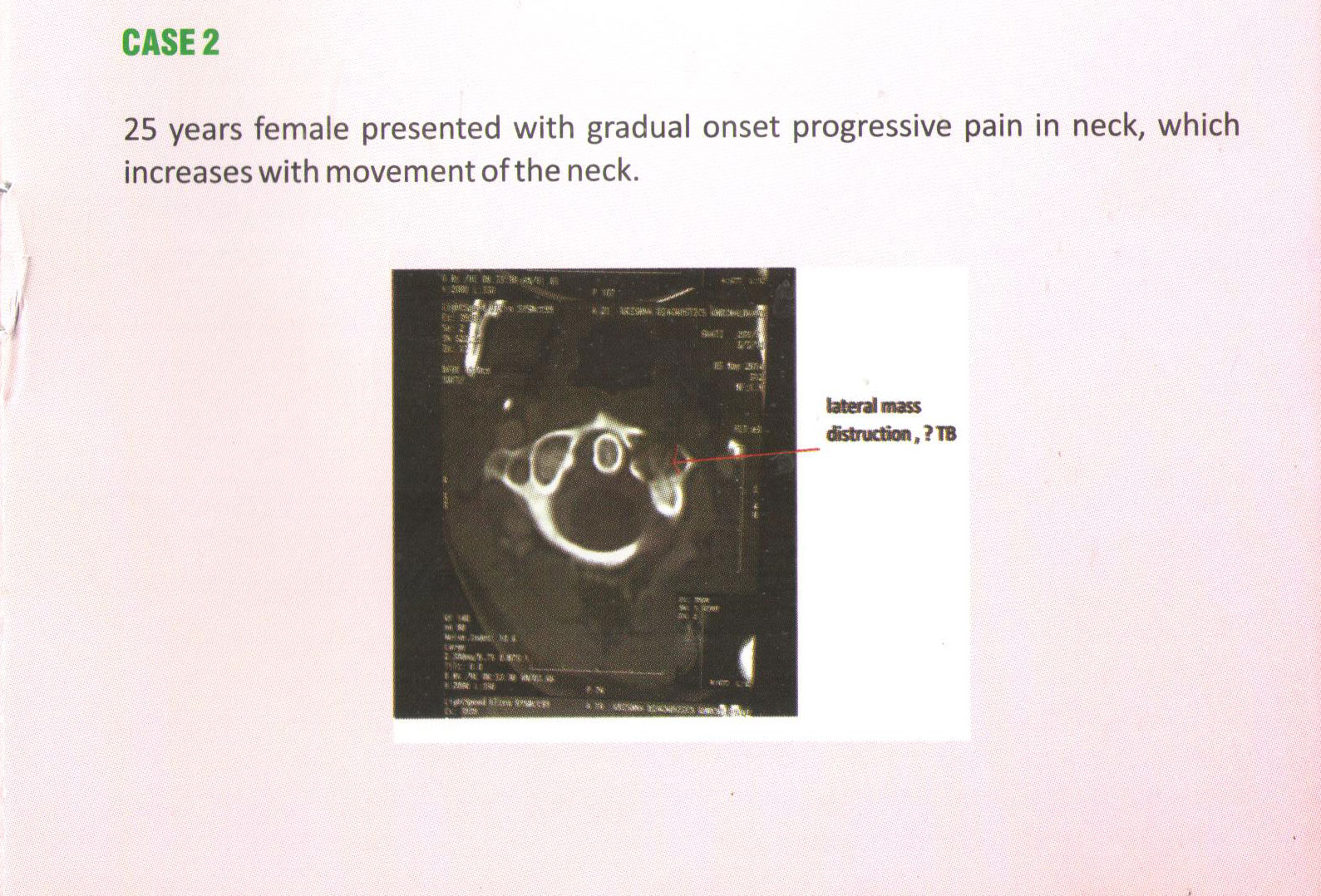
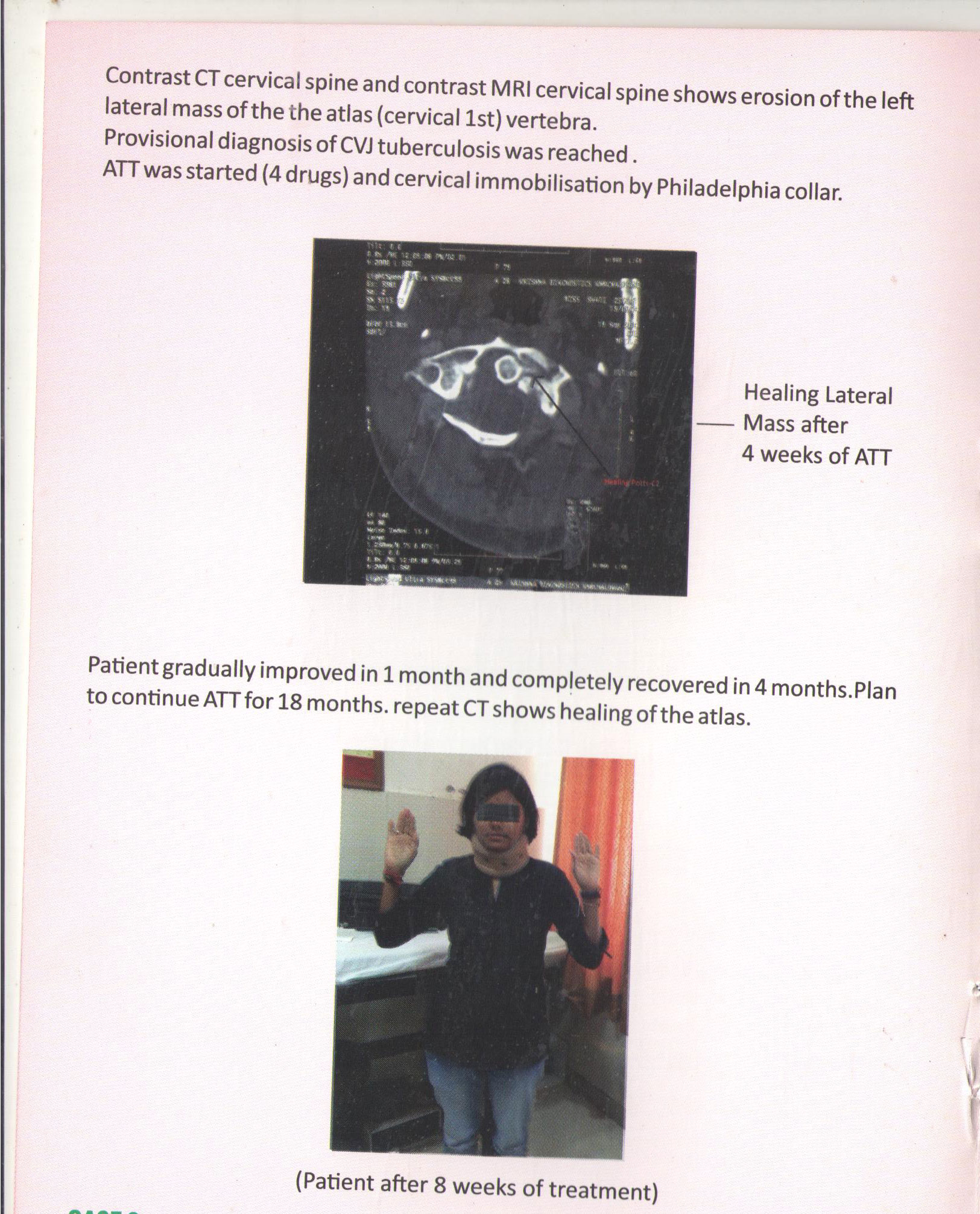
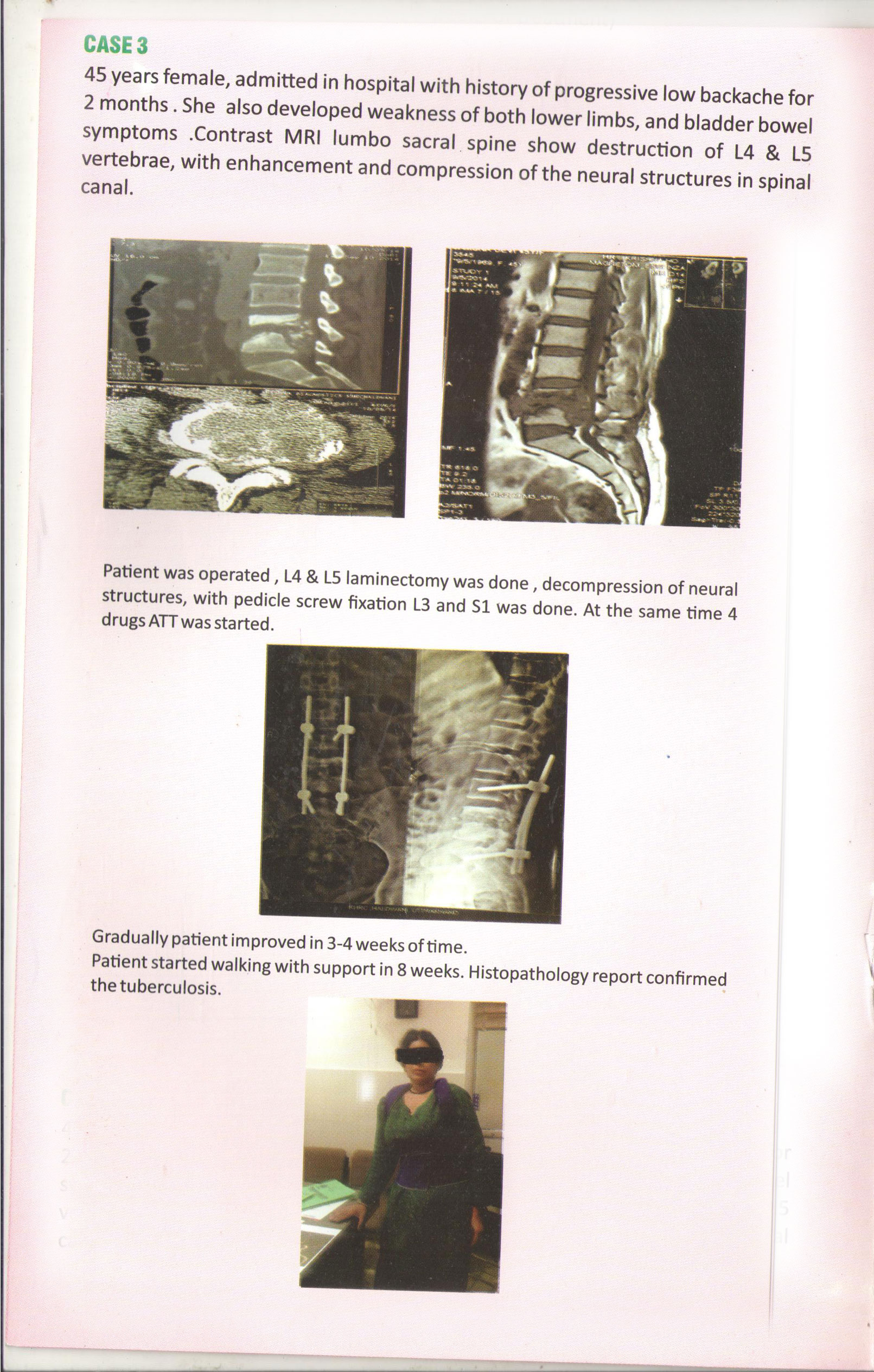
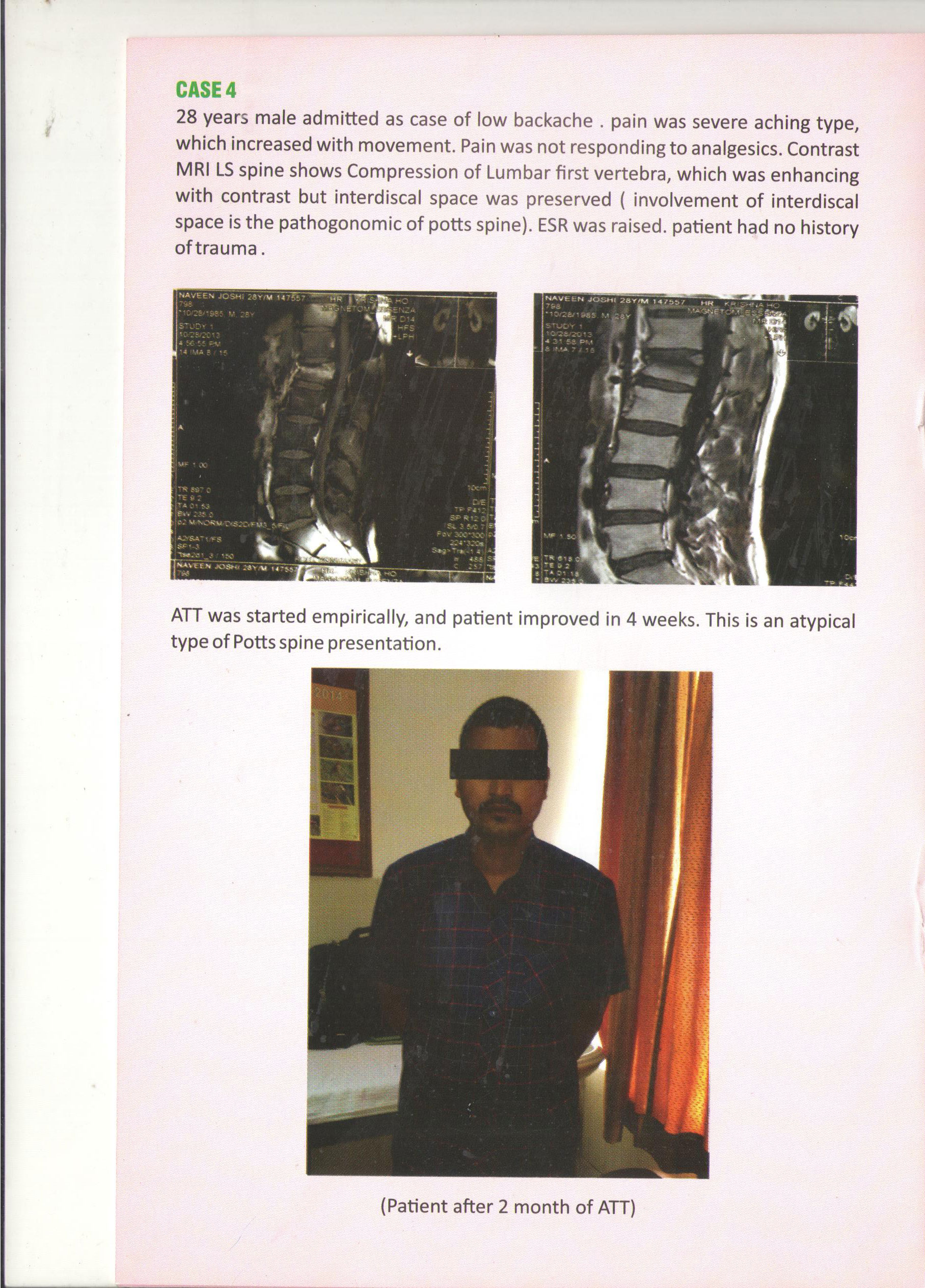
50 yrs male presented with complain of Headache, seizures, vomiting Left hemi paresis, drowsiness Contrast MRI brain show right fronto parietal abscess . Patient was operated and abscess was drained, Patient recovered well.
MRI BRAIN of patient showing abscess in brain
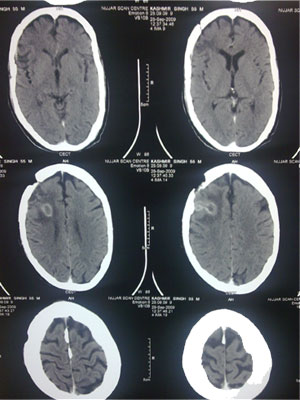
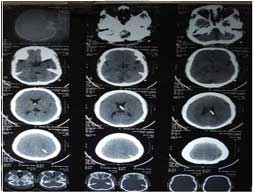
CT head of patient after surgery
Patient walking 1 day after surgery

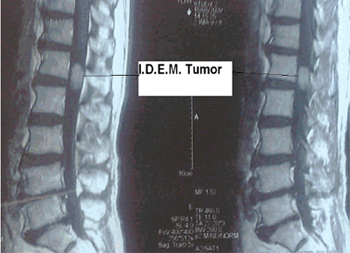
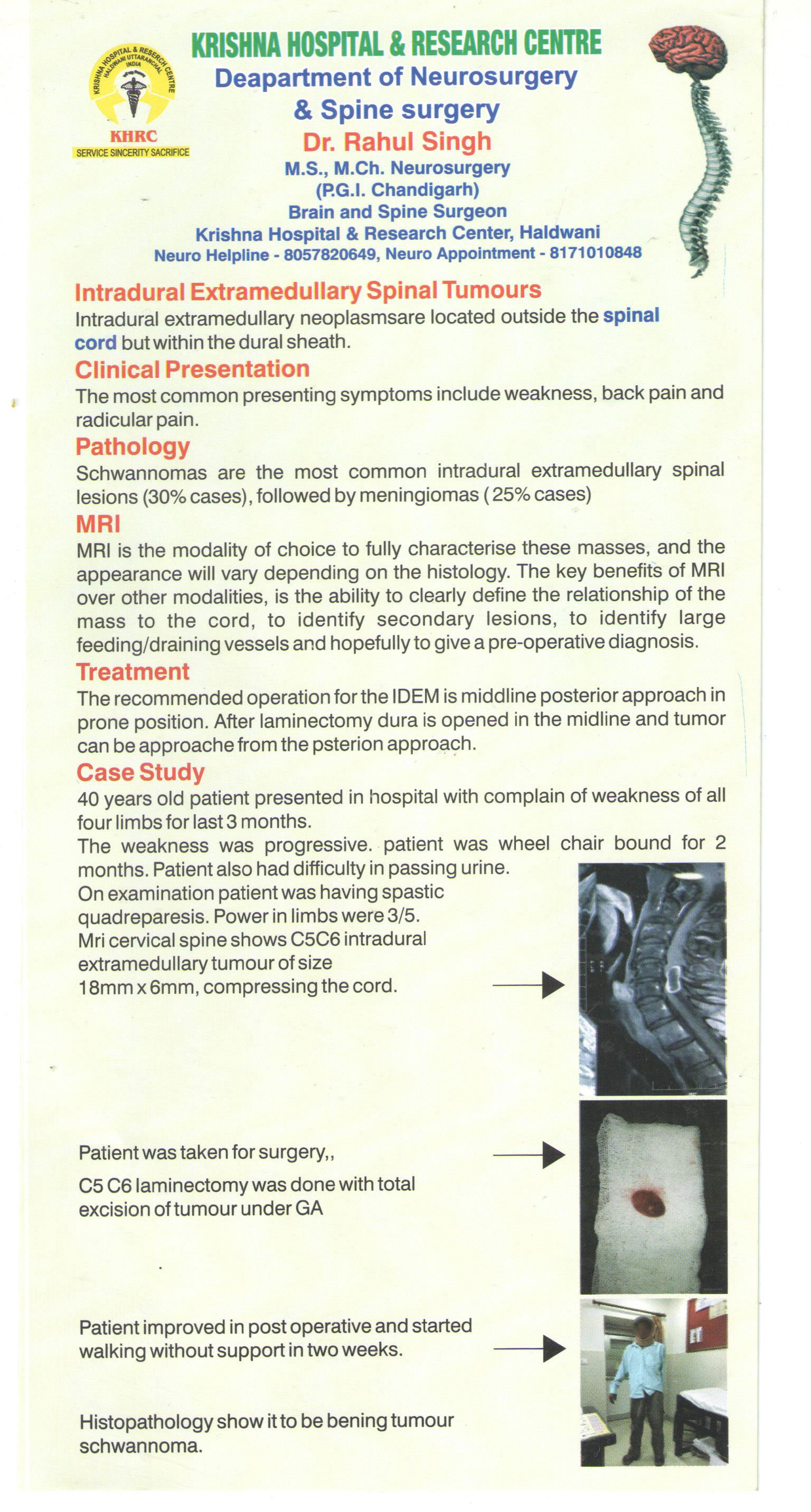
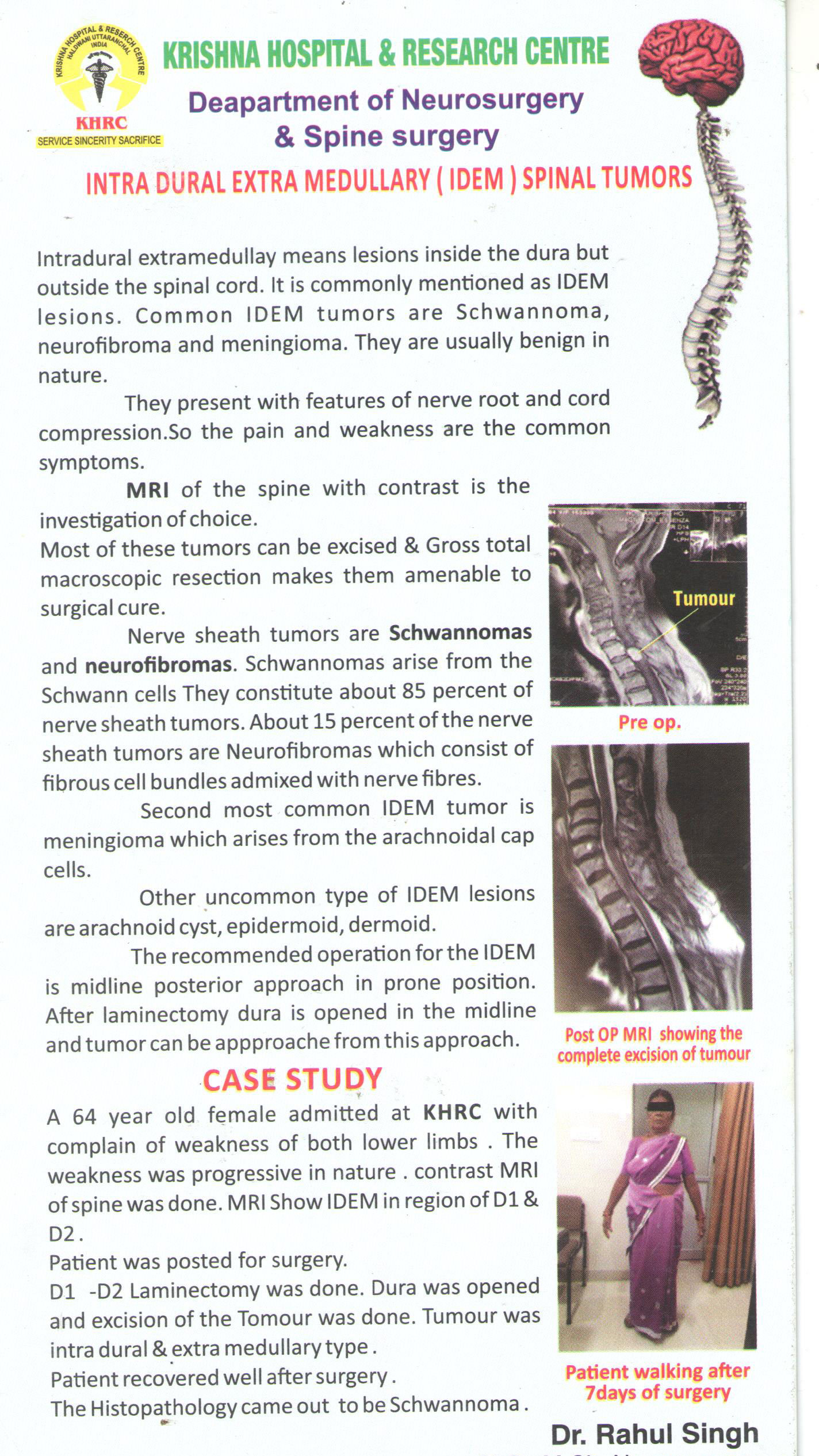
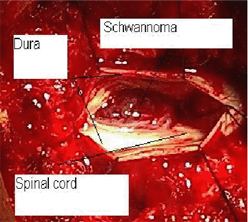
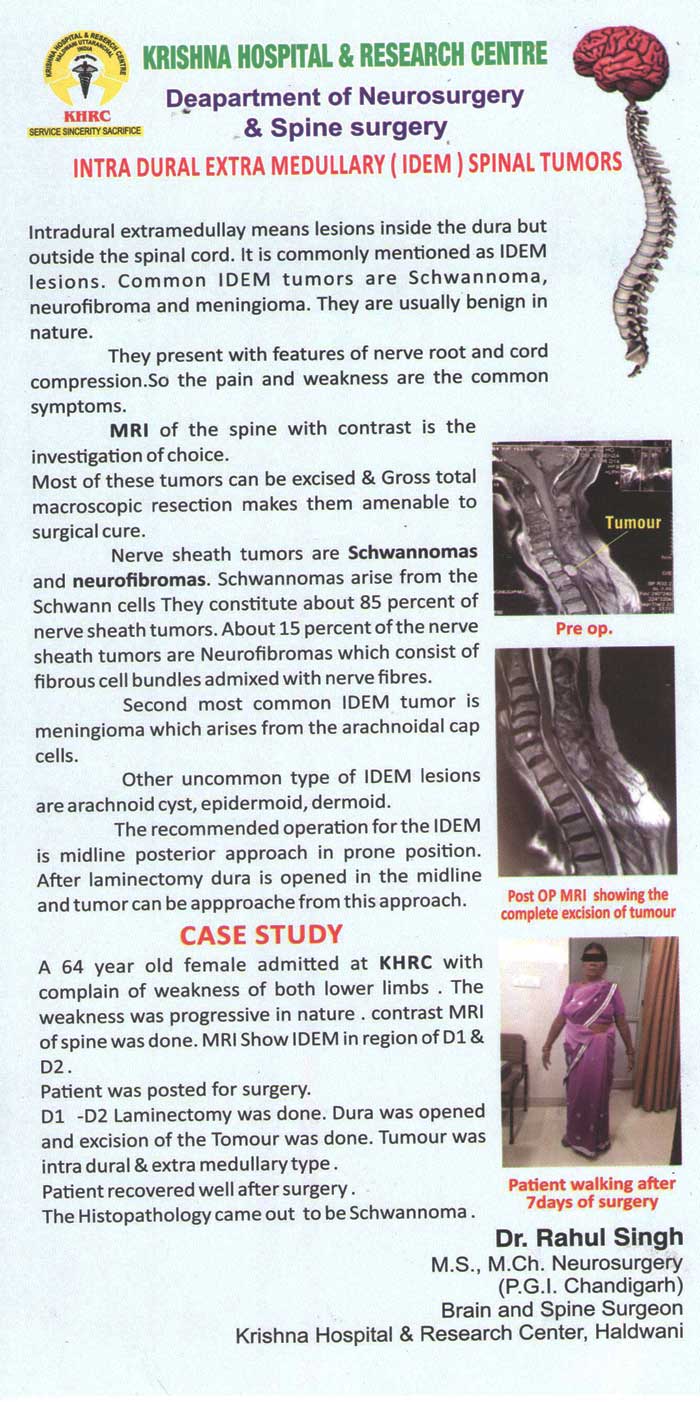
On MRI spine there was a intra dural extramedullary tumor at L1 level compressing the spinal cord and displacing it towards one side.
65 years old male patient presented with history of backache and numbness and weakness of both lower limbs for last 6 months. There was on improvement with medicines he has taken from local doctor .
Laminectomy done at L1 level , dura opened, cord and tumor identified and total excision of tumour done in one piece.



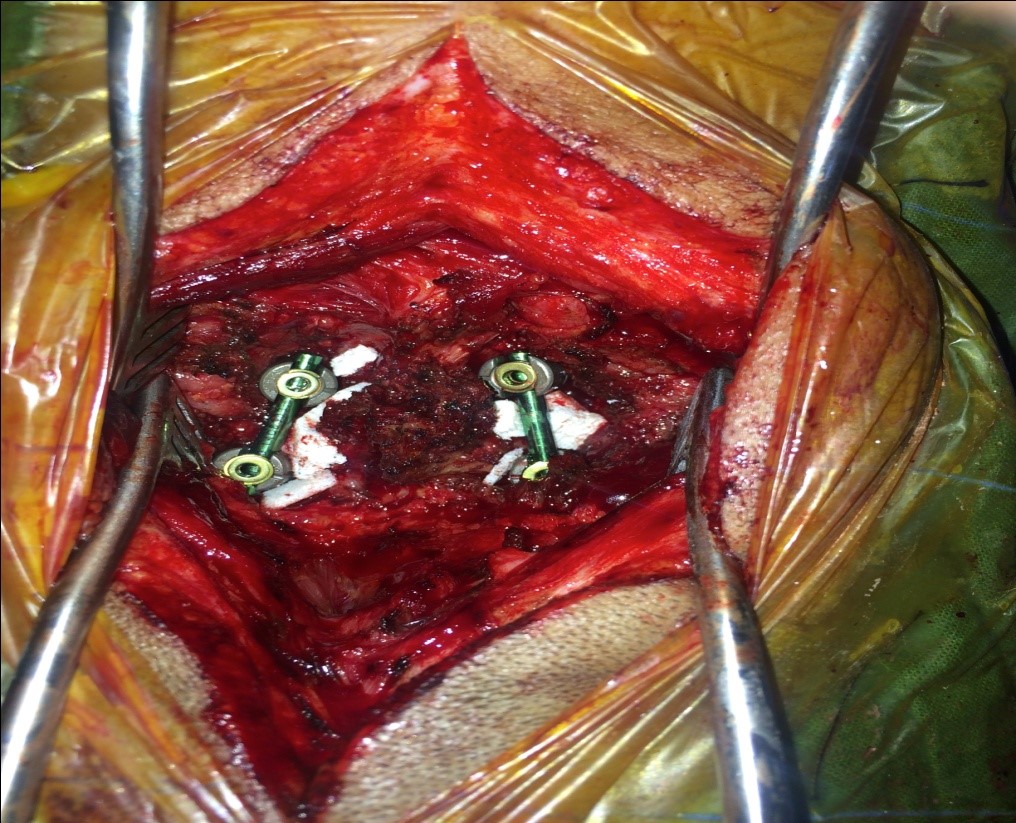
Patient was operated for L1 Spine fracture. Decompression of spinal cord with pedicle screw fixation eas done.
23 years female fall from height , patient suffered from Lumbar first fracture with weakness of both legs.
Patient was operated for L1 Spine fracture.

Patient was operated for L1 Spine fracture.
Patient had good recovery and started walking on 7th post op day.

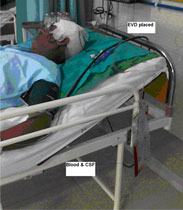
Immediately right frontal burr hole was made and external ventricular drain was placed.
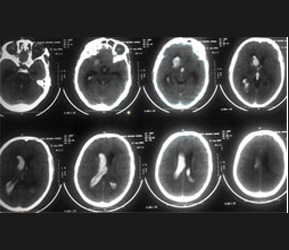
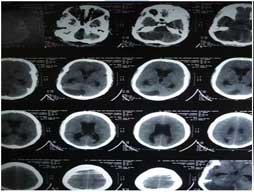
55 yrs Male Patient admitted with history of sudden unconsciousness , GCS on arrival was E1V1M4. NCCT head show massive intraventricular Haemorrhage , more on right lateral ventricle.
Patient improved gradually. After few days EVD was converted to Ventricular Peritoneal( V P) shunt.
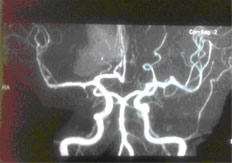
Brain angiogram was normal.
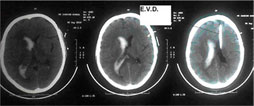
Patient regained consciousness after 10 days.
discharged in satisfactory condition.


Pre Op MRI Cervical Spine
55 yrs male Complain of gradual onset progressive weakness of all 4 limbs with pain in cervical reigon. On CT and MRI found to have severely compressed cervical cord at cervical 5,6 & 7 levels due to ossified posterior longitudinal ligament(OPLL). Patient had tried conservative treatment in form of physiotherapy, analgesics, shartwave diathermy, cervical collar , but was not relieved.
Cervical cord compression a C5 C6 & C7 Level.
Patient was operated at K.H.R.C. Anterior approach was taken, after cervical 6 corpectomy the ossified posterior longitudinal ligament was completely resected under operating microscope, thus compression from spinal cord relieved. Bone graft was placed and secured with titanium plate and screws Post op patient starting improving and after 2 weeks he was 90% relieved of his symptoms of spasticity , pain , numbness and weakness.





Prolapse intervertebral disc
Prolapse intervertebral disc is a very common problem , it affects the persons of every age group in both sexes. Lumbar region especially L4-L5 and L5-S1 is most commonly affected. Cervical disc protrusion with nerve compression is next most common. Patient usually complain of backache or cervical pain with radiation to limb depending upon which nerve is compressed. In era of minimal invasive surgery protruded vertebral disc which are compressing the nerve are dissected out through microneurosurgical technique with help of operating microscope.
Advantages of Microdiesctomy are
- 1. Small incision small scar.
- 2. Less of tissue dissection so less pain .
- 3. Surgery done under 300 times magnification so the spinal cord and nerves can be saved from accidental injuries during surgery.
- 4. more precision during surgery.
- 5. Less hospital stay ( Usually 3 days).
- 6. Early mobility. Patient can walk on next day after surgery.





Gun Shot injury in head
35 yrs male had a gunshot wound in head left frontal reigon with bullet penetrating the skull and lodging in brain parenchyma, leaving the wound open and brain mater coming out and patient was comatose.
Emergency surgery done at K.H.R.C. , bullet taken out, debridement , bone repair, haemostasis was done. Patient recovered later.






Elderly female came to K.H.R.C. emergency in drowsy state.
Patient improved by next day.
Patient improved by next day.
Patient two months after surgery.

20 years old male presented with complain of cervical pain for 4 months, gradually progressive,with numbness and tingling sensations in upper limbs & spasticity of lower limbs.
MRI cervical spine shows cervical 5 vertebral body collapse, cause??
Patient was given cervical traction followed by surgery , anterior cervical approach was taken, cervical 5 corpectomy was done , bone grafting & plating done.


Patient gradually improved. Patient became symptoms free after 1month.
Histopathology confirmed tuberculocis. Antitubercular treatment was given for 18 months.

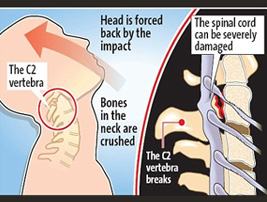
HANGMAN FRACTURE
INTRODUCTION
Hangman’s fractures have been used to describe traumatic spondylolisthesis of C2. It is defined as fractures to the lamina, articular facets, pedicles, or pars of the axis vertebra. involves the pars interarticularis of C2 on both sides, and is a result of hyperextension and distraction. Hangman’s fractures are often caused by falling, diving or motor vehicle accidents.
Clinical presentation
Post-traumatic neck pain after hyperextension high velocity injury is the most common presentation. Neurological impairment is seen only in 25% of patients.
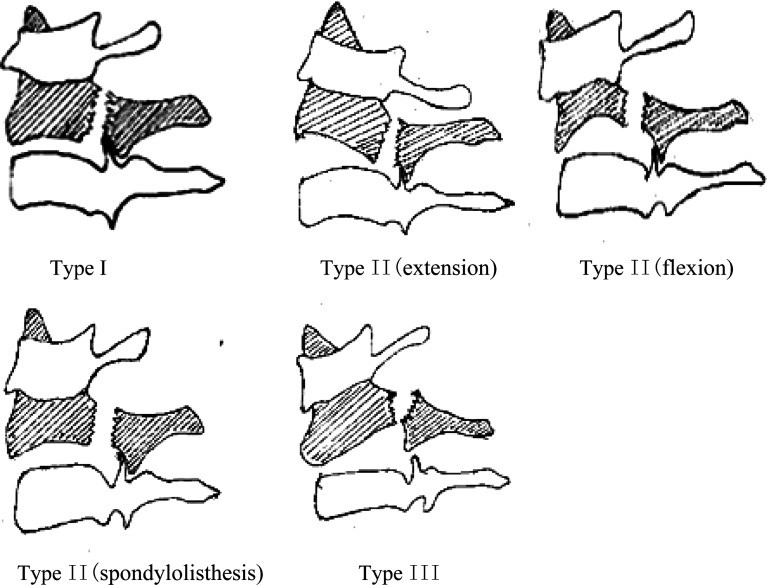
Types of Hangman Fracture
MANAGEMENT
Type 1 conservative, cervical collar, Halo collar. Surgery might be the primary method to Levine-Edwards Type II, IIa and III fractures.
CASE:-
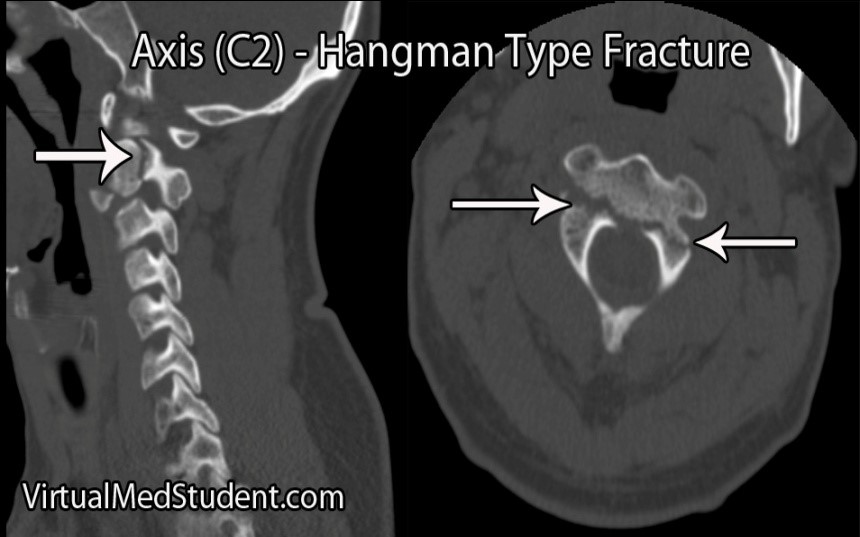
40 Years old man admitted in KHRC with history of high velocity impact road traffic accident 1 day back. Patient complain was severe cervical pain, which increase on movement of the neck.
X-Ray Cervical spine and C.T. Cervical spine was done with shows traumatic spondylolisthesis of C-2.
Type II (flexion),
Patient was given rigid cervical collar.
Patient was operated on day 3, after giving cervical traction C-2, C-3 Lateral mass screw fixation was done.
Patient was given rigid cervical

Patient was operated on day 3,
Post op Period was uneventful.

Post op X-rays.

Patient free of symptoms (Post op day 14th)


Spine Surgery
36 years old female admitted at Krishna Hospital Haldwani with complain of Severe radicular pain in the left upper limb. MRI cervical spine was done, it shows for prolapse intervertebral disc at C5 and C6 level compressing the left C6 nerve root . Patient was taken for minimal invasive spine surgery under general Anaethesia . C5 and C6 nerve root on the left side was decompressed under microscope . Patient was completely relieved from pain and was discharged two days later




Case at neurosurgery DEPT at Krishna Hospital
12 years male child admitted in emergency room of Krishna hospital with complain of weakness of both lower limbs and difficulty in micturition , with sudden increase in weakness of both lower limbs . On examination the power of left lower limb was 2/5 and right lower limb was 3/5,, with bladder and bowel involvement. Contrast MRI Spine shows large cyst( 10 mm x 5 mm) in dorsal spinal cord at D3 and D4 level. the cyst was intramedullary in position and compressing the cord to thin rim . surgery was planned under general anaesthesia in prone position. D3 D4 laminectomy was done and cord was opened (myelotomy) in midline and cyst was excised in toto under operating microscope. Postop period was uneventful. Child slowly started gaining power in lower limbs. After two months he is able to walk without support with regaining of bladder and bowel functions. Histopathology shows cyst with columnar ciliated epithelium consistent with neuroentric / enetrogenous / endodermal cyst. post op MRI shows total excision of cyst.




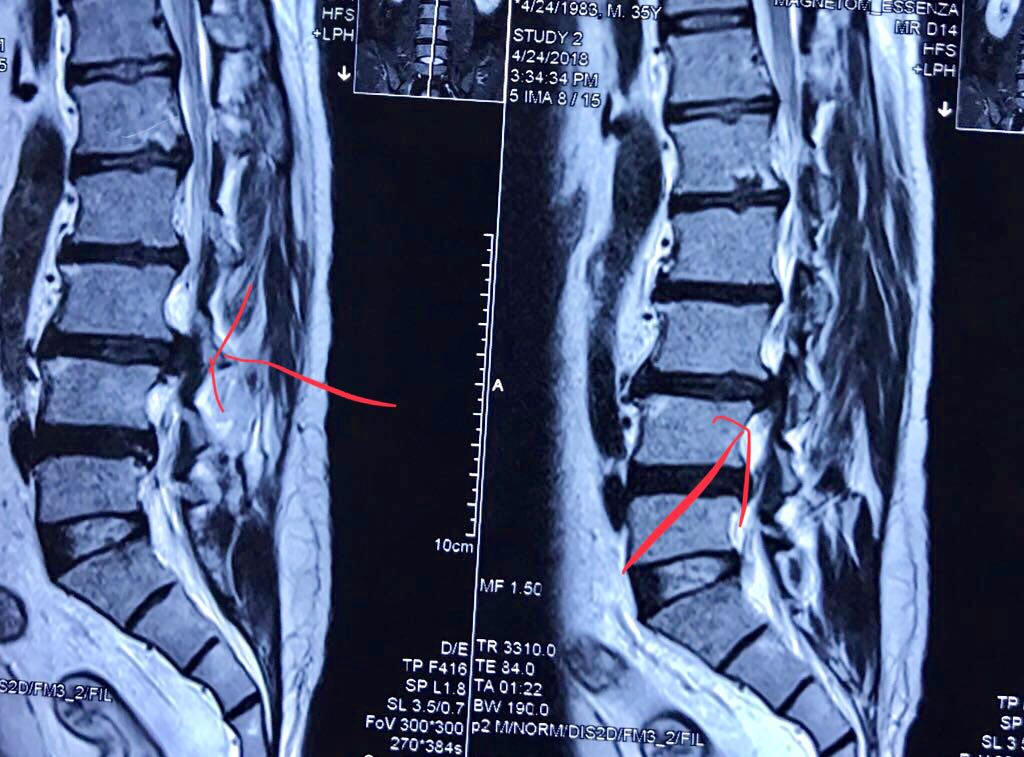
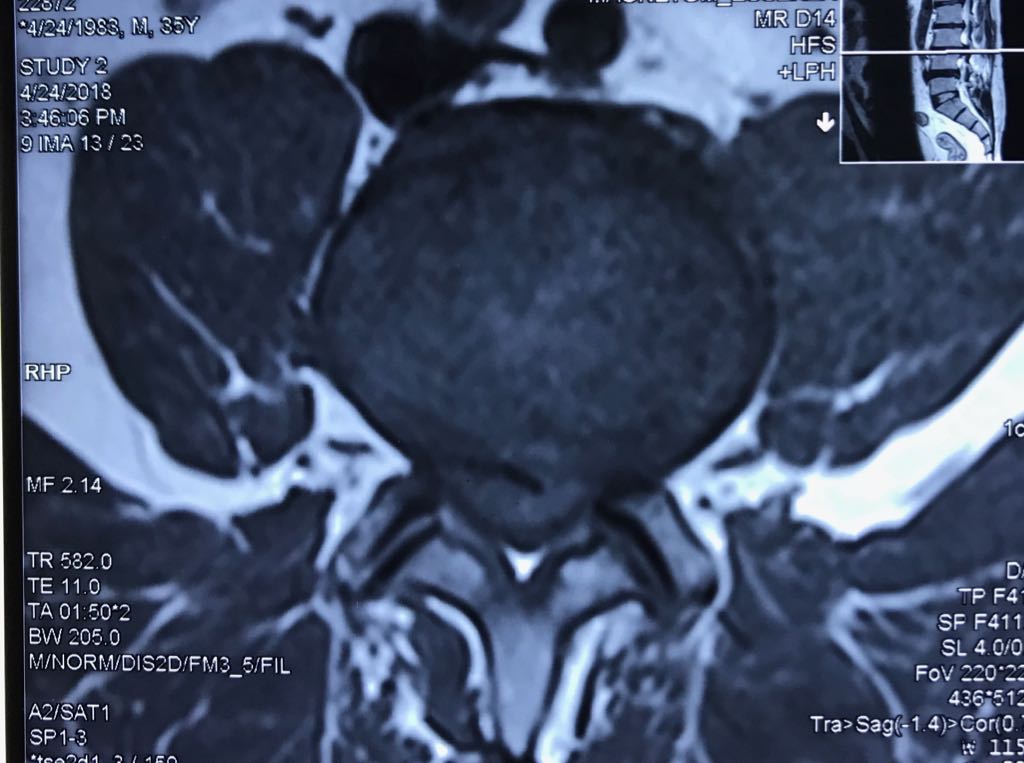
Severe Back Pain Radiating to Both Lower Limbs and Inability to Pass Urine
35 years young male admitted in KRISHNA Hospital with complain of sudden severe back pain radiating to both lower limbs and inability to pass urine (cauda equina syndrome) . MRI shows extruded L3L4 disc. Urgent microdiectomy L3-L4 done by Dr Rahul Singh Neurosurgeon. Patient improved after surgery